

Frontier Systems Technical Paper
Company-Led Technical Preprint / Technical Disclosure Version
Version 1.0 | 2026
From Labour Substitution to High-Value Care Transformation: The Mathematical Extension of the RR-Care™ Framework for Humanoid Eldercare Robots
Weijie Tan 1,†, Wentao Zhao 1,†, Qiang Huang 1, Xin Zhao 1, Hon Hsiang Ong 1, Tingting Shen 2, Tian Shen 1, Chunqiu Yan 2, and Jian Zhang 1,*
¹ AJJ Healthcare Management Pte. Ltd., Singapore.
² Hangzhou Huaxi Intelligent Technology Co. Ltd., Hangzhou, China.
† These authors contributed equally to this work and share first authorship.
* Correspondence: zhangjian@ajjmedtech.com.sg
Important Notice
This document is a company-led public research version prepared for transparent disclosure, public reference and subsequent scholarly discussion. It has not yet undergone independent peer review and should not be interpreted as a peer-reviewed journal article, regulatory approval, clinical validation, government endorsement, institutional endorsement, investment recommendation, sales forecast, staffing-reduction authorisation or evidence of universal deployment readiness.
Publication and Evidence Boundary
This AJJ Research public version is intentionally shorter than the full peer-reviewed journal manuscript under preparation. It summarises the RR-Care™ extensional framework logic, the FTE 2.3 released-care baseline, FTE-based care-capacity interpretation, high-value care transformation logic and evidence-control approach, while withholding detailed source-record traceability files, supplementary materials, full calculation worksheets, site-level raw evidence and reviewer-facing methodological details.
Prior Public Version and Future Journal Submission Boundary
This public version may be further developed into a substantially revised manuscript for peer-reviewed journal submission. Any subsequent journal submission should disclose this public version and its website URL or DOI in accordance with the target journal’s policy. For journal submission, the manuscript should retain additional scholarly value, including fuller literature anchoring, methodological explanation, supplementary evidence materials, calculation worksheets and transparent disclosure of this prior public version.
Abstract
Institutional eldercare systems face increasing pressure from population ageing, nursing workforce shortages, night-shift burden, repetitive task demands and rising expectations for safe, continuous and person-centred care. Humanoid eldercare robots may support selected routine tasks and release caregiver workload, but their value should not be interpreted only as labour substitution or staffing reduction. This AJJ Research public version presents a company-led frontier systems technical paper that mathematically extends the RR-Care™ framework from a baseline Full-Time Equivalent released-care estimate into a high-value care transformation model.
The paper introduces HVCI, a High-Value Care Transformation Index designed to examine how the RR-Care™ FTE 2.3 released-care baseline may be converted into higher-value nursing and eldercare capacity through deliberate workflow redesign. In this framework, FTE 2.3 is not treated as a fixed law, regulatory benchmark, clinical outcome, universal staffing standard or automatic replacement of 2.3 nurses or caregivers. Rather, it is interpreted as a context-specific, framework-derived released-care baseline under defined institutional assumptions.
The model distinguishes between released care capacity and converted high-value care capacity, using a conversion coefficient to assess whether freed caregiver time is redirected toward relational care, individualized observation, family communication, professional judgement, staff micro-rest and other human-centred activities. It further integrates care quality improvement, human-robot collaboration and friction or regression cost into a structured decision-support logic. The purpose is to evaluate whether robotic workload release becomes usable nursing and eldercare value, rather than remaining a theoretical efficiency figure.
This public research version is intended to provide a transparent, time-stamped technical disclosure of the HVCI framework for public reference and future scholarly discussion. It does not constitute independent peer review, clinical validation, regulatory approval, medical device certification, staffing-reduction authorisation, institutional endorsement or evidence of universal deployment readiness. The full journal manuscript under preparation is expected to contain fuller literature anchoring, methodological explanation, supplementary evidence materials, calculation worksheets and reviewer-facing evidence-control details.
Keywords: Humanoid eldercare robot; FTE 2.3; RR-Care™; HVCI; high-value care transformation; nursing workflow redesign; human-robot collaboration; institutional eldercare; care-capacity release; evidence-control framework
1. Introduction
1.1 Background: From Caregiver Shortage to Robotic Care Capacity
Global population ageing places immense pressure on long-term care systems, creating a structural mismatch between service demand and available caregiving labour[1]. Humanoid eldercare robots offer a technological response by assisting with routine, repetitive, and physically burdensome tasks, thereby releasing human caregivers to focus on higher-value activities. The initial RR-Care™ study introduced a computational framework to calculate the replacement ratio (Full-Time Equivalent, FTE) of these robots. However, determining FTE savings is only the first step. The critical second-stage question is how this released FTE is systematically transformed into high-value care capacity, such as empathy, judgement, and individualized attention.
1.2 Why FTE Calculation Alone Is Not Enough
While FTE calculation provides essential quantifiable evidence for institutional planning, it remains an incomplete measure of robotic value. A narrow focus on labour substitution risks reducing eldercare to mere cost-saving, neglecting the irreplaceable human elements of emotional reassurance, ethical responsibility, and professional judgement. Robots excel at programmable, routine support, whereas humans are essential for complex communication and moral judgement[2]. Therefore, FTE calculation must serve as the mathematical starting point for a second-order analytical model: converting labour substitution into high-value care transformation to improve care quality and staff wellbeing.
1.3 Research Objective and Contribution
This paper develops a mathematical extension of the RR-Care™ framework[3], shifting from a one-dimensional labour-substitution result to a multidimensional high-value care transformation model. It makes four primary contributions. First, it establishes a conceptual distinction between FTE release (labour capacity made available) and FTE value conversion (the extent to which this capacity is redirected toward higher-value care). Second, it proposes a transformation logic where released time is systematically reallocated to emotional support, individualized planning, and staff micro-rest. Third, the study introduces an integrated extension model that logically links released FTE, high-value care conversion, human-robot collaboration, care quality, and friction costs. Finally, it advances the RR-Care™ pathway as a pioneering, norm-shaping framework for evaluating the economic and social value of robotic deployment in institutional care[4][5].
1.4 Structure of the Paper
The remainder of this paper is structured to logically unfold this transformation model. Section 2 clarifies the relationship with the initial RR-Care™ framework, while Section 3 reviews existing literature on eldercare robotics and labour substitution. Sections 4 and 5 develop the theoretical framework and apply it to specific institutional scenarios. Section 6 presents the mathematical extension pathway, followed by the data validation design in Section 7. Finally, Sections 8 through 11 discuss broader institutional implications, summarize the research contributions, address methodological limitations, and conclude the study.
2. FTE 2.3 as a Released-Care Baseline
2.1 Summary and Baseline Function of the First RR-Care™ Framework
The first RR-Care™ study established a foundational computational framework for evaluating the replacement ratio of care robots in elderly care institutions[3]. Its central contribution was translating robot-supported workload into measurable indicators, including Full-Time Equivalent (FTE) impacts, economic value, and workforce transition implications. By providing a “first-definition-type” structure, it offered a standardized metric to assess staffing pressure and deployment feasibility. However, interpreting this metric narrowly as headcount reduction is incomplete and misleading. Because essential elements of care—such as emotional reassurance and ethical judgment—remain inherently human, the present study treats the initially derived FTE reduction not as a final conclusion, but as an analytical baseline. The focus therefore shifts to a second-stage inquiry: how this released labour capacity is systematically redirected and transformed into essential qualitative activities, such as personalized care planning, profound resident observation, and caregiver recovery time.
2.2 From Labor Substitution to Strategic Value Transformation
Transitioning from mechanical labour substitution to strategic value transformation requires recognizing that offloading routine tasks to robots does not automatically generate institutional value[5]. The resulting FTE reduction merely creates a pool of potential capacity. Realizing this potential demands the active reallocation of released caregiver time toward empathy-driven roles, supported by disciplined workflow redesign, staff training, and robust institutional governance. Consequently, this study develops a mathematical and operational extension of the initial framework. By systematically accounting for conversion efficiency, care quality improvement, human-robot collaboration, and friction adjustments, it dismantles job displacement fears and repositions robots as essential collaborative tools. Ultimately, this research provides an evidence-oriented infrastructure that links baseline labour substitution with a multidimensional transformation logic, guiding operators and policymakers in the responsible, human-centric deployment of eldercare robotics.
3. Literature Review and Research Gap
3.1 Fragmented Perspectives in Existing Literature
Existing literature on eldercare robotics predominantly focuses on functional assistance and basic labour substitution without systematically evaluating how released capacity is redirected into high-value nursing and eldercare activity. While foundational studies, including the initial RR-Care™ framework, successfully translated task performance into measurable Full-Time Equivalent (FTE) metrics, a central research gap remains: the absence of an integrated mathematical framework explaining how this released FTE is systematically converted into high-value care. Currently, research streams spanning functional robotics, interaction studies, care quality, and economic evaluation remain largely isolated, failing to provide a cohesive institutional transformation model.
3.2 Bridging the Gap: HCI, CQI, and Socio-Economic Integration
To bridge these disconnected streams, this study extends the foundational framework by introducing multidimensional transformation variables[7]. First, while traditional Human-Robot Interaction (HRI) studies emphasize usability and social acceptance, they often overlook how robotic integration fundamentally alters care workflows. This study shifts the focus to care-oriented Human-Robot Collaboration (HRC), introducing the Human-Robot Collaboration Index (HCI) to measure task reallocation efficiency[2][7]. Second, qualitative care studies prioritize emotional support and personalization but rarely link these critical outcomes to operational capacity[8][9][10]. By introducing Care Quality Improvement (CQI) as an explicit analytical variable, this research structures how offloading repetitive tasks indirectly enhances human-delivered relational care. Finally, unlike narrow economic evaluations focused strictly on immediate labour savings, this model positions high-value care transformation as the critical bridge connecting operational efficiency with broader socio-economic impacts, such as reduced caregiver burnout and sustainable care delivery.
3.3 Comparative Research Gap Synthesis
The integrated approach developed in this study moves beyond isolated metrics, providing a structured mechanism to evaluate robotic deployment as essential infrastructure for human-centred institutional care. This paradigm shift from isolated literature streams to an integrated transformation model is synthesized in Table 1.

4. Theoretical Framework: FTE High-Value Care Transformation Model
Figure 1 is inserted at this point to provide a visual bridge between the baseline FTE release logic and the high-value care transformation model. It should be read as the public technical-paper architecture of HVCI: FTE 2.3 remains the released-care baseline, while the model evaluates how that released capacity may be converted into higher-value nursing and eldercare capacity through workflow redesign, quality improvement, human-robot collaboration and friction adjustment.

Figure 1. Conceptual architecture of the HVCI high-value care transformation model.
The figure illustrates how the RR-Care™ FTE 2.3 released-care baseline is first converted into high-value care capacity through FTE (HVC) = FTE (R) × θ, and then integrated with QCI, HCI and FRC to form the HVCI decision-support index. To avoid double counting, is treated as the released-care baseline and is not added again as an independent positive term in the final HVCI formula. The framework is an academic and operational model, not clinical validation, regulatory approval, medical device certification or universal deployment authorisation.
Accordingly, Section 4 defines each component of the visual architecture: released care capacity, high-value care conversion, care quality improvement, human-robot collaboration, operational friction and the integrated HVCI extension logic.
4.1 Released and High-Value Care Capacity
The model begins with released care capacity (FTE (R)), strictly quantifying the human-equivalent workload freed when robots assume routine tasks. Because merely releasing time does not guarantee human-centred value, this baseline serves as a prerequisite starting point. The framework subsequently defines high-value care capacity (FTE (HVC)) as the specific fraction of successfully redirected toward relational, cognitive, or supervisory activities. This transformation is governed by a conversion coefficient (θ), formulated as . Constrained within , this mathematical distinction prevents the flawed assumption that all labour substitution inherently translates into optimal care reallocation.
4.2 Care Quality and Collaboration Mechanisms
To evaluate transformation effectiveness, the model introduces two critical adjustment variables. The Care Quality Improvement Index (QCI) captures qualitative enhancements such as timeliness, emotional reassurance, and dignity preservation. It explicitly avoids technological determinism by acknowledging that poorly integrated deployment can induce alert fatigue, potentially negating care quality. Concurrently, the Human-Robot Collaboration Index (HCI) evaluates workflow synergy. Moving beyond general user acceptance, HCI measures whether robotic support tangibly improves task coordination, staff allocation, and workflow continuity rather than acting as isolated automation.
4.3 Operational Friction and Regression Cost
Acknowledging that real-world deployment is never completely frictionless, the framework incorporates Friction and Regression Cost (FRC). This variable captures unavoidable inefficiencies, technical downtimes, and additional supervisory burdens. Functioning as a necessary negative adjustment, rigorously defends against technological optimism by explicitly penalizing poorly managed deployments characterized by weak coordination and rewarding strong institutional readiness.
4.4 Integrated FTE Extension Logic
Finally, the integrated extension logic synthesizes these multidimensional variables to construct the composite High-Value Care Transformation Index (HVCI). To avoid double counting, the released-care baseline is not added again as an independent positive term in the final index, because converted high-value care capacity is already expressed as FTE (HVC) = FTE (R) × θ. To eliminate dimensional inconsistency across heterogeneous metrics, all components are standardized before integration:
where FTE (HVC) represents converted high-value care capacity, QCI represents care quality improvement, HCI represents human-robot collaboration, and FRC represents friction and regression cost. The positive weighting coefficients are subject to the constraint:
The friction coefficient λ is treated as a separate penalty coefficient rather than a positive contribution weight. These coefficients allow the framework to adapt to varying institutional priorities, such as workforce sustainability, care-quality improvement, collaboration reliability and deployment friction. Ultimately, this second-order framework evaluates whether measurable released-care capacity is intentionally converted into usable, human-centred nursing and eldercare value.
5. Scenario-Based Transformation Logic
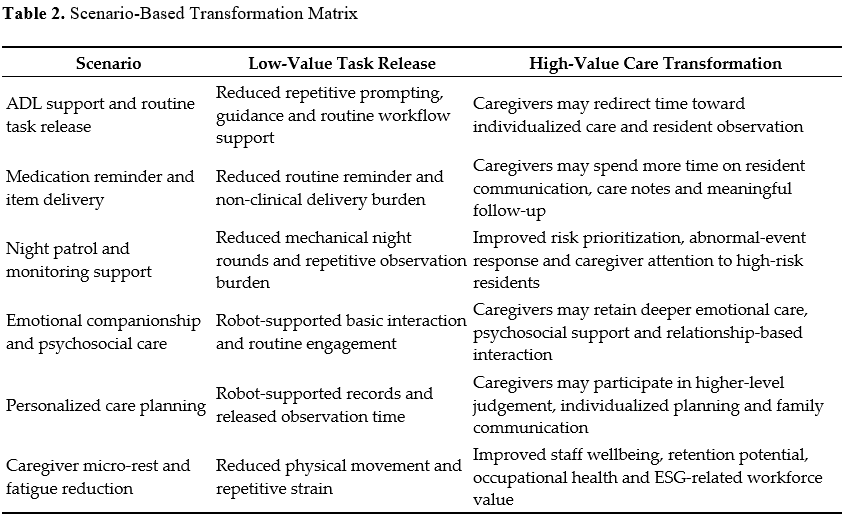
5.1 Routine Workflows and Delivery Support
Humanoid robots offloading Activities of Daily Living (ADL) support, non-clinical deliveries, and scheduled reminders systematically generate baseline released capacity (FTE (R)). This strategic substitution mitigates physical burdens, such as caregiver walking time and repetitive prompting. However, this theoretical release achieves institutional value only when actively redirected into high-value capacity (FTE (HVC)), governed by the conversion coefficient (θ). If robotic routing is unreliable or generates false alerts, anticipated workload savings are proportionally negated by operational friction (FRC). Crucially, automated reminders merely assist institutional workflows and categorically do not replace professional clinical oversight.
5.2 Night Patrol and Emotional Companionship
In night-shift scenarios, robots performing mechanical patrols create a layered monitoring structure that directly mitigates caregiver burnout. While this generates , it demands a robust Human-Robot Collaboration Index (HCI) to enforce explicit task boundaries and prevent dangerous over-reliance on automated anomaly detection. Similarly, robots can provide baseline emotional engagement, but they cannot substitute human empathy. By absorbing basic interaction needs, robots indirectly generate , enabling caregivers to focus on complex psychosocial support. Elevating the Care Quality Improvement Index (QCI) in these domains strictly requires empirical verification and rigorous ethical escalation boundaries.
5.3 Personalized Care Planning and Workforce Wellbeing
Transforming released time into personalized care planning exemplifies optimal utilization, allowing caregivers to detect subtle behavioral shifts often missed under severe operational strain. Furthermore, strategically offloading routine burdens facilitates caregiver micro-rest, mitigating burnout and systematically elevating through sustained attention and responsiveness. This human-centred value inherently drives Environmental, Social, and Governance (ESG) workforce resilience. Yet, poorly implemented systems demanding continuous human correction sharply increase , actively exacerbating fatigue.
5.4 Comparative Scenario Transformation Matrix
The utility of humanoid robots extends beyond simple task substitution; each domain represents a distinct pathway where automated efficiency must be deliberately converted into human care capacity. This scenario-based logic is synthesized in Table 2.
6. Mathematical Extension and Calculation Pathway
6.1 Baseline Release and High-Value Conversion
The mathematical extension systematically transitions from first-order labour substitution to second-order value transformation. It begins with the baseline release (FTE (R)), strictly quantifying the human-equivalent capacity liberated through routine task substitution. Functioning solely as an initial input, does not represent ultimate institutional value. The second analytical step determines the proportion of this capacity successfully redirected toward higher-value care, governed by the conversion coefficient (θ). Defined formally as FTE (HVC) = FTE (R) x θ (where 0 ≤ θ ≤1 ), this step demands rigorous empirical substantiation, such as time-motion analyses. This is crucial because high baseline release yields minimal transformational value if institutional reallocation remains fundamentally weak.
6.2 Quality Conversion and Collaboration Indices
To measure observable outcomes—such as response timeliness and individualized planning—the third step introduces the Care Quality Improvement Index (QCI). To prevent dimensional inconsistency when integrated with capacity units, undergoes standard min-max normalization:
This yields a standardized variable (QCI - circumfix ) scaled strictly between 0 and 1. Finally, the fourth step evaluates operational efficacy through the Human-Robot Collaboration Index (HCI). Moving decisively beyond superficial hardware usability, rigorously assesses task-boundary clarity, escalation protocols, and role redesign. Standardized as HCI - circumfix, it acts as a critical adjustment factor. A low score indicates systemic collaborative friction that forces staff into continuous remedial oversight, thereby severely eroding the theoretical gains of automated capacity release.
7. Data Validation Design and Evidence Boundary
7.1 Purpose and Evidence Architecture
The Data Validation Report establishes an auditable evidence-control framework to operationalize the model's multidimensional variables (FTE (R), FTE (HVC), QCI-circumfix , HCI-circumfix, and FRC-circumfix). Crucially, it functions strictly as a research-support instrument, explicitly distinct from clinical diagnoses, regulatory certifications, or universal deployment approvals. To substantiate the mathematical model, empirical data is organized into a structured architecture. Task-level and capacity-reallocation records form the foundational tiers, quantifying baseline release and grounding the conversion coefficient (θ) in observed institutional behaviour. Concurrently, care-quality, collaboration, and friction evidence serve as essential adjustment variables, ensuring qualitative enhancements and operational interruptions are rigorously documented rather than theoretically assumed.
7.2 Data Protection and Interpretation Boundaries
Given the sensitive nature of care environments, the validation design rigorously adheres to data minimization and anonymisation principles, excluding all personally identifiable information (PII) to ensure full ethical compliance. Furthermore, the framework operates within a strictly defined evidence boundary. Core variables are inherently context-sensitive, necessitating site-specific calibration based on institutional layout and governance readiness. This mathematical evaluation explicitly does not supersede professional clinical oversight; human caregivers retain absolute authority over resident safety and escalation procedures. Ultimately, while providing a robust analytical infrastructure, the framework remains a theoretical model requiring multi-site empirical validation, independent peer review, and longitudinal assessment.
8. Discussion
8.1 From Labor Substitution to Human-Centred Care Enhancement
The central argument of this study is that the derived FTE metric must not be interpreted merely as a labour-substitution figure. While the foundational RR-Care™ framework established a method to estimate released human-equivalent workload, this study addresses the second-order question: how this released capacity converts into higher-value, sustainable care. Eldercare cannot be reduced to mechanical task completion; it relies heavily on emotional reassurance, professional judgement, and dignity preservation. Therefore, the value of robotic deployment lies not in eliminating human presence, but in systematically reorganizing capacity. By reframing deployment as a human-centred enhancement mechanism, this model directly challenges fears of dehumanization, demonstrating that robotic value depends entirely on an institution’s ability to preserve and elevate empathy-driven human care.
8.2 Implications for Institutional Eldercare Operators
For operators, this mathematical extension shifts robotic deployment from a simple equipment purchase to a strategic workflow redesign exercise. Instead of asking only if a robot reduces workload (FTE (R)), operators must evaluate whether that time is intentionally reallocated (FTE (HVC) ) toward personalized planning or family communication. If institutions fail to deliberately manage this reallocation, the transformation coefficient (θ) remains low, and theoretical savings vanish into administrative friction. This model provides a practical, layered assessment structure—evaluating QCI-circumfix , HCI-circumfix, and FRC-circumfix enabling disciplined deployment reviews, robust budget planning, and data-driven board-level communication.
8.3 Implications for Workforce Transition and ESG Value
This framework carries profound implications for workforce transition and Environmental, Social, and Governance (ESG) value. By strategically offloading repetitive tasks, humanoid robots allow caregivers to transition toward supervisory, relational, and individualized roles. This role upgrading directly addresses severe occupational challenges such as night-shift pressure and emotional burnout. Within the social dimension of ESG, reducing physical strain and enabling caregiver micro-rest fosters a resilient, sustainable workforce. However, this human-centred value is not automatic. The model explicitly incorporates Friction and Regression Cost (FRC-circumfix) to warn that poorly implemented technology—causing alert fatigue or supervision ambiguity—actively weakens ESG value. Thus, workforce transition is framed not as labour displacement, but as essential labour reallocation.
8.4 Norm-Shaping Framework and Multi-Dimensional Integration
Together, the initial RR-Care™ study and this mathematical extension establish a pioneering evaluation chain, transitioning from labour substitution to high-value care transformation. By creating a standardized evaluative language that connects operational efficiency with socio-economic value, this research serves as a cautious, evidence-based, and norm-shaping framework in the emerging field of eldercare robotics. Importantly, this model functions as a single operational pillar within a broader architecture comprising RR-Gov™ (governance readiness) and RR-Ethics™ (accountability and dignity). The transformation model quantifies the value-conversion layer but does not substitute for ethical or governance oversight. Ultimately, this integrated ecosystem underscores that mechanical workload release is only one facet of a responsible, human-centric deployment strategy that requires multi-site empirical validation and strict clinical oversight.
9. Research Contribution and World-First-Type Positioning
9.1 First-Definition-Type and Mathematical Contributions
The initial RR-Care™ study established a pioneering, “first-definition-type” framework for mathematically evaluating robotic labour substitution and baseline Full-Time Equivalent (FTE) impact. The present study represents a substantive, second-stage “world-first-type” contribution by advancing this pathway from mere labour measurement to high-value care transformation. Rather than asking how much labour a robot can release, this mathematical extension asks how effectively that released capacity is transformed into human-centred institutional value. It achieves this by structurally separating released workload (FTE (R)), converted care value (FTE (HVC) , governed by the conversion coefficient (θ), and realized institutional impact. By integrating qualitative and operational variables—namely the Care Quality Improvement Index (QCI), the Human-Robot Collaboration Index (HCI), and Friction and Regression Cost (FRC)—into the composite High-Value Care Transformation Index (HVCI), this layered architecture successfully prevents the flawed assumption that robotic task substitution automatically equates to care improvement.
9.2 Institutional Deployment Contribution
Practically, this framework translates robotic labour substitution into actionable care-management logic. It clarifies for institutional operators that robotic deployment must be approached as a comprehensive workflow redesign rather than a standalone equipment purchase. The model provides a structured, sequential deployment review architecture: institutions first assess theoretical baseline release (FTE(R)), evaluate deliberate capacity reallocation ( FTE (HVC) and θ), and subsequently adjust for operational realities using QCI, HCI and FRC. This structured evaluation empowers operators to identify whether weak deployment outcomes stem from low conversion efficiency, poor collaborative integration, or excessive operational friction, thereby guiding pilot design, staff training, and continuous operational monitoring.
9.3 Pioneer Developer Context: AJJ × Huaxi
The AJJ × Huaxi programme provides an essential, applied developer context for this theoretical framework, treating humanoid eldercare robotics not merely as laboratory concepts but as institutional care technologies requiring rigorous governance and workflow evaluation. Crucially, this developer context is utilized to conceptually refine the RR-Care™ pathway, not to serve as a commercial endorsement or universal proof of deployment success. It highlights that as eldercare robotics mature toward real-world institutional application, stakeholders demand auditable, transparent evaluation models rooted in evidence control and independent academic scrutiny rather than superficial functional claims.
9.4 Cautious Boundary of the World-First-Type Claim
The “world-first-type” positioning of this research is maintained as a strictly cautious, evidence-based academic claim rather than an absolute assertion of global uniqueness. While prior studies have independently examined eldercare robotics, labour substitution, and human-robot interaction, the pioneering significance of this pathway lies in its integrated architectural definition. Together, the foundational RR-Care™ study and the present mathematical extension form a distinctive, auditable research pathway. They systematically unite robotic replacement ratios, FTE conversion, and friction-sensitive deployment logic to mathematically define how routine capacity release can be demonstrably transformed into sustainable, high-value institutional care.
10. Limitations and Future Research
10.1 Boundary of Assumptions and Multi-Site Validation
The proposed high-value care transformation model is subject to critical limitations. Firstly, the baseline capacity relies on the foundational RR-Care™ assumptions and does not represent a universally fixed metric. Outcomes fluctuate significantly based on context-specific variables such as facility layout, resident dependency, and workforce training maturity. Consequently, the derived baseline and the transformation coefficient ( ) measure potential operational pathways rather than guaranteed outcomes; their actualization depends entirely on deliberate institutional management. Secondly, to ensure broad applicability, the model necessitates extensive multi-site validation. Future research must apply this framework across diverse settings—including nursing homes and community care centres—to systematically document how core variables (FTE(R), FTE(HVC), QCI, HCI, FRC, and HVCI ) behave under varying staffing pressures and technological adoption conditions.
10.2 Independent Validation and Multi-Dimensional Integration
Thirdly, the model requires rigorous independent external validation. To mitigate internal bias, independent care operators, clinical advisors, and governance experts must evaluate both the mathematical coherence and empirical traceability of the framework. It is paramount to reiterate that this operational evaluation does not constitute clinical validation, regulatory approval, or medical device certification. Finally, future research must deeply integrate this operational model with broader governance and ethical readiness frameworks, specifically RR-Gov™ and RR-Ethics™. Evaluating deployment value is fundamentally incomplete without ensuring robust data protection, continuous human oversight, and legal accountability. A deployment yielding substantial FTE (R) or FTE (HVC) remains inadequate if ethical boundaries or institutional governance controls fail. Therefore, longitudinal studies are essential to verify that released capacity is consistently converted into measurable, ethically governed, and institutionally sustainable care value.
11. Conclusion
11.1 Summary and Contribution to Care Transformation
This study successfully extends the foundational RR-Care™ framework, transforming the calculated Full-Time Equivalent metric from a simple labour-substitution outcome into a multidimensional high-value care transformation model. By explicitly distinguishing the baseline capacity released through routine task substitution (FTE (R)) from the portion actively converted into human-centred care (FTE (HVC)), the mathematical extension confirms that calculated capacity release is merely the analytical starting point. Because high-value eldercare fundamentally relies on human judgment, empathy, and ethical sensitivity, this model reframes robotic deployment as a strategic enabler of qualitative care transformation rather than a narrow cost-reduction exercise.
11.2 Institutional Norms and Final Statement
Furthermore, this research contributes to institutional deployment norms by providing a structured evaluation language for operators, developers, and researchers. It mandates that institutions move beyond measuring theoretical workload reduction to rigorously evaluate whether saved time is intentionally reallocated, governed by variables such as the conversion coefficient (θ), Care Quality Improvement Index (QCI), Human-Robot Collaboration Index (HCI), and operational friction (FRC). While this theoretical framework necessitates future multi-site empirical validation and integration with broader governance and ethical models, it establishes a pioneering, auditable two-stage pathway. Ultimately, this framework affirms that the true value of humanoid eldercare robotics lies not in replacing human staff, but in enabling institutions to systematically redesign workflows so that caregivers can dedicate more time to empathetic, professional, and sustainable relational care.
Declarations
Author Contributions:
Conceptualization, Jian Zhang; methodology, Weijie Tan, Wentao Zhao, Qiang Huang and Jian Zhang; formal analysis, Weijie Tan, Wentao Zhao; investigation, Weijie Tan, Wentao Zhao, Qiang Huang, Chunqiu Yan and Tingting Shen; data curation, Wentao Zhao, Qiang Huang and Tingting Shen; framework development, Weijie Tan, Wentao Zhao, Qiang Huang and Jian Zhang; writing-original draft preparation, Weijie Tan, Wentao Zhao and Qiang Huang; writing-review and editing, Xin Zhao, Hon Hsiang Ong, Tingting Shen, Tian Shen, Chunqiu Yan and Jian Zhang; supervision, Jian Zhang and Chunqiu Yan; project administration, Jian Zhang. Weijie Tan and Wentao Zhao contributed equally to this work and share first authorship. All authors have read and agreed to the public research version of this document.
Funding:
This research received no external funding.
Institutional Review Board Statement:
The research described in this public version focuses on the mathematical extension of the RR-Care™ framework and theoretical workflow reallocation assessment within institutional elderly care environments. It constitutes an operational, workflow and capacity-transformation evaluation rather than a clinical intervention study involving diagnosis, treatment or medical decision-making. Field-supported assessment of the transformation variables, including θ, QCI, HCI and FRC, is based on aggregated robotic telemetry, anonymised operational records and non-invasive time-motion observations of standard caregiver workflows under institutional permission or internal approval where applicable. No identifiable resident medical records, biometric identification data or individual clinical decision data are disclosed in this public research version.
Informed Consent Statement:
Not applicable. This public research version introduces a mathematical framework and scenario-based transformation logic. It does not disclose identifiable resident-level clinical data, individual medical decision-making, facial images, voice recordings, biometric identifiers or personally identifiable information. Any referenced operational workflows or caregiver capacity reallocations, including , are discussed exclusively in aggregated, theoretical or anonymised forms.
Data Availability Statement:
The multidimensional high-value care transformation logic and mathematical extensions described in this public version are supported by internally retained anonymised source-record traceability files. These include system-log summaries, baseline released-care capacity calculations, conversion coefficient θ calibration materials and standard variable scaling matrices for QCI, HCI and FRC. The detailed supporting mathematical, operational and evidence-control files are retained by the Company for confidentiality, data-protection and institutional anonymity reasons and are not published with this public research version. Where appropriate, supporting materials may be made available to journal editors or qualified reviewers under suitable confidentiality and data-protection arrangements.
Supplementary Materials:
The full S1–S3 supplementary evidence package, including the FTE 2.3 high-value care transformation data validation report, expanded HVCI nursing workflow redesign tables, nursing decision-support scoring worksheet, calculation-support materials, dimensional normalisation logic and scenario-based operational evidence files, is not published with this company-led public research version. These materials are retained for controlled academic review, evidence-control, source-record traceability and future peer-reviewed journal submission. They do not constitute clinical validation, regulatory approval, medical device certification, proof of guaranteed care-quality improvement, staffing-reduction authorisation or universal deployment evidence. Successful institutional transformation remains context-dependent and requires local calibration, independent review and multi-site validation where appropriate.
Acknowledgments:
The authors acknowledge the participating elderly care institutions, frontline caregivers, technical deployment personnel, and operational support teams involved in the AJJ × Huaxi program, whose practical insights into humanoid eldercare robotics helped conceptually refine this mathematical extension and scenario-based transformation logic. No government, regulatory, or institutional endorsement is implied by this acknowledgment.
Conflicts of Interest:
Some authors are affiliated with AJJ Healthcare Management Pte. Ltd. and Hangzhou Huaxi Intelligent Technology Co., Ltd., which are involved in the development, deployment, or technical-support context of the humanoid eldercare robotics discussed in this public research version. This document is a company-led public research version presenting an evaluative mathematical framework. It should not be construed as independent third-party validation, regulatory approval, clinical validation, medical device certification, commercial endorsement, or a guarantee that mechanical workload release automatically converts to high-value care without deliberate institutional management.
Ethics and Evidence Boundary Statement:
This public research version presents a framework-level mathematical extension and field-supported operational assessment. It does not report a clinical trial, patient-level outcome study, medical diagnosis, treatment intervention, or individual healthcare decision-making evaluation. The proposed integration of operational efficiency with socio-economic variables should be interpreted as preliminary, context-specific, and evidence-bounded support for the second-stage RR-Care™ framework, strictly subject to independent peer review, multi-site empirical validation, and local institutional recalibration.
Declaration of AI-Assisted Language and Editorial Support:
AI-assisted language and editorial tools may have been used to support English language refinement, grammar checking, formatting consistency and document readability. The authors retained full responsibility for the study design, data interpretation, mathematical framework, evidence boundaries, intellectual content and final document. No AI tool was used to independently generate, alter or verify the underlying source data, institutional records or empirical findings described in this public research version.
REFERENCES
-
World Health Organization (2020) Decade of Healthy Ageing: Baseline Report. World Health Organization, Geneva.
-
Broadbent, E., Stafford, R. and MacDonald, B. (2009) Acceptance of Healthcare Robots for the Older Population: Review and Future Directions. International Journal of Social Robotics, 1, 319-330. https://doi.org/10.1007/s12369-009-0030-6
-
Zhao, W., Huang, Q., Zhao, X., Ong, H.H., Tan, W., Yan, C., Shen, T.T., Shen, T. and Zhang, J. (2026) A Theoretical Framework for Calculating the Replacement Ratio of Care Robots in Elderly Care Institutions: Algorithm Development and Preliminary Validation. Health, in press.
-
Donabedian, A. (1988) The Quality of Care: How Can It Be Assessed? JAMA, 260, 1743-1748. https://doi.org/10.1001/jama.1988.03410120089033
-
Drummond, M.F., Sculpher, M.J., Claxton, K., Stoddart, G.L. and Torrance, G.W. (2015) Methods for the Economic Evaluation of Health Care Programmes. 4th Edition, Oxford University Press, Oxford.
-
Broekens, J., Heerink, M. and Rosendal, H. (2009) Assistive Social Robots in Elderly Care: A Review. Gerontechnology, 8, 94-103.
https://doi.org/10.4017/gt.2009.08.02.002.00 -
Macalupu, V., Miller, E., Martin, L. and Caldwell, G. (2025) Human-Robot Interactions and Experiences of Staff and Service Robots in Aged Care. Scientific Reports, 15, Article No. 2495. https://doi.org/10.1038/s41598-025-86255-w
-
Dall’Ora, C., Ball, J., Reinius, M. and Griffiths, P. (2020) Burnout in Nursing: A Theoretical Review. Human Resources for Health, 18, Article No. 41. https://doi.org/10.1186/s12960-020-00469-9
-
Pu, L., Moyle, W., Jones, C. and Todorovic, M. (2019) The Effectiveness of Social Robots for Older Adults: A Systematic Review and Meta-Analysis of Randomized Controlled Studies. The Gerontologist, 59, e37-e51. https://doi.org/10.1093/geront/gny046
-
Moyle, W., Cooke, M., Beattie, E., Jones, C., Klein, B., Cook, G. and Gray, C. (2013) Exploring the Effect of Companion Robots on Emotional Expression in Older Adults with Dementia: A Pilot Randomized Controlled Trial. Journal of Gerontological Nursing, 39, 46-53. https://doi.org/10.3928/00989134-20130313-03