

Public-Facing Q&A for Government Agencies, Eldercare Institutions, Medical Professionals, Engineers, Investors and Interested Readers
RR-Care™ FTE 2.3: A First-Definition-Type Care-Capacity Release Framework for Multi-Functional Embodied AI Humanoid Eldercare Robotics
Related DOI: 10.5281/zenodo.20774293
DOI URL: https://doi.org/10.5281/zenodo.20774293
Document type of related paper: Company-led DOI-registered frontier systems technical paper / technical disclosure
Status of related paper: Public research version; not independently peer-reviewed; not a journal article or final peer-reviewed publication
Status of this Q&A
This Q&A is a public-facing explanatory note prepared to help readers understand the RR-Care™ framework and its related technical paper. This Q&A itself is not a peer-reviewed journal article, regulatory filing, clinical validation report, medical-device certification document, staffing-reduction authorisation, commercial valuation or investment recommendation.
Executive Summary
RR-Care™ FTE 2.3 is a public-facing explanatory framework for understanding how selected robot-supported routine care tasks may release caregiver workload capacity in institutional eldercare settings.
The illustrative FTE = 2.3 estimate is a framework-derived, context-specific workload-release planning indicator under defined assumptions. It should not be interpreted as one robot replacing 2.3 caregivers, clinical validation, regulatory approval, product certification, staffing-reduction authorisation, commercial valuation or universal deployment readiness.
This Q&A is intended to help government agencies, eldercare institutions, medical professionals, engineers, investors and public readers understand the purpose, methodology, evidence boundary and interpretation limits of the related RR-Care™ technical paper.
Table 1. Correct Interpretation versus Incorrect Interpretation of RR-Care™ FTE 2.3
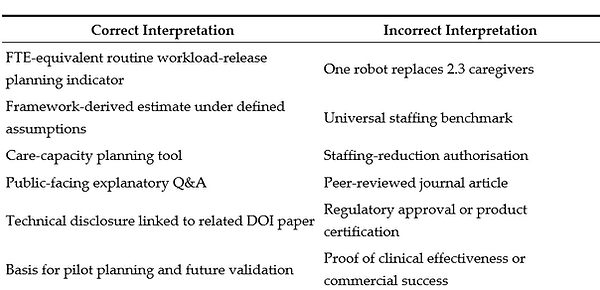
Purpose of this Q&A
This Q&A is prepared as a public-facing explanatory note for readers of the RR-Care™ framework and related AI-enabled eldercare robotics research. It is intended to help government agencies, healthcare and eldercare institutions, medical professionals, engineers, governance reviewers, investors and other interested readers understand the purpose, scope, methodology, evidence boundary and interpretation limits of the RR-Care™ framework.
RR-Care™ should be understood as a company-led, non-peer-reviewed research paper, technical disclosure and planning framework for estimating robot-supported routine workload-release capacity in institutional eldercare settings. It should not be interpreted as clinical validation, regulatory approval, medical-device certification, product clearance, government endorsement, institutional endorsement, staffing-reduction authorisation, investment advice, commercial valuation or universal deployment permission.
1. What is RR-Care™?
Q1. What is the purpose of the RR-Care™ framework?
RR-Care™ is a framework-level research and planning model designed to evaluate how robot-supported routine care activities may release caregiver workload capacity in institutional eldercare settings.
The framework does not claim that a robot directly replaces a caregiver. Instead, it converts selected robot-supported routine task activity into an FTE-equivalent workload-release planning indicator under defined assumptions, human supervision and institutional workflow boundaries.
In simple terms, RR-Care™ asks:
If certain routine, repeatable and supervised care-support tasks are assisted by a robot, how much caregiver routine workload may be released for higher-value human care, supervision, resident interaction or operational redeployment?
RR-Care™ is therefore a planning, workload-analysis and governance-support framework. It is not a clinical validation result, not regulatory approval, not medical-device clearance, not product certification and not staffing-reduction authorisation.
2. What exactly does RR-Care™ measure?
Q2. What is the exact output measured by the RR-Care™ framework?
The principal output of RR-Care™ is an estimated FTE-equivalent routine workload-release capacity.
This means the framework estimates the amount of routine caregiver time that may be released when selected robot-supported tasks are performed under defined conditions. The output is expressed as an FTE-equivalent planning indicator, not as a direct headcount replacement claim.
RR-Care™ does not measure or prove:
-
clinical outcome improvement;
-
resident health improvement;
-
medical treatment effect;
-
regulatory approval;
-
medical-device clearance;
-
guaranteed staffing reduction;
-
caregiver redundancy;
-
commercial revenue;
-
sales forecast;
-
investment return;
-
universal deployment readiness;
-
universal safety.
The output should be interpreted as:
a framework-derived, context-specific estimate of routine workload-release capacity under defined task, time, workflow, supervision and demand assumptions.
3. What does FTE mean in RR-Care™?
Q3. What is meant by FTE-equivalent workload release?
FTE means full-time equivalent. In RR-Care™, it is used as a planning unit to express the amount of routine caregiver workload that may be released under defined assumptions.
It does not mean that a robot automatically replaces a full-time caregiver. It means that certain robot-supported routine tasks may reduce the amount of human time needed for selected routine activities, allowing caregiver capacity to be reallocated to supervision, interaction, documentation, safety monitoring, resident engagement or other higher-value care tasks.
The correct interpretation is:
FTE-equivalent workload release is a planning indicator for released routine workload. It is not a direct staff-replacement figure.
4. What is the meaning of FTE = 2.3?
Q4. What does the illustrative FTE = 2.3 estimate mean?
The RR-Care™ framework identifies an illustrative FTE-equivalent routine workload-release estimate of approximately 2.3 FTE per robot per year under defined demonstration assumptions.
This number must be interpreted carefully.
It does not mean:
-
one robot replaces 2.3 caregivers;
-
2.3 staff can be removed;
-
staffing reduction is guaranteed;
-
the number applies to all institutions;
-
the number has been clinically validated;
-
the number is a regulatory benchmark.
The safer interpretation is:
The RR-Care™ framework derives an illustrative FTE-equivalent routine workload-release estimate of approximately 2.3 FTE per robot per year under defined task-support, operating-hour, demand-constraint and human-supervision assumptions.
This figure is a framework-level planning indicator. It is subject to recalibration depending on local workflow, actual utilisation, task mix, operating hours, caregiver work patterns, supervision burden, facility layout, resident profile, institutional policy and governance controls.
5. Is FTE = 2.3 a universal conversion factor?
Q5. Can the FTE = 2.3 estimate be used as a universal benchmark?
No.
The FTE = 2.3 figure should not be treated as a universal conversion factor or staffing benchmark. It is an illustrative estimate derived under defined framework assumptions.
Different institutions may have very different results depending on:
-
resident profile;
-
facility layout;
-
task mix;
-
robot operating hours;
-
caregiver workflow;
-
supervision requirements;
-
incident escalation protocols;
-
maintenance burden;
-
training requirements;
-
technology reliability;
-
local regulatory and institutional rules.
The correct public interpretation is:
FTE = 2.3 is an illustrative, framework-derived workload-release estimate under defined assumptions. It must be recalibrated before being applied to any specific institution.
When used appropriately, the FTE = 2.3 estimate may support preliminary pilot planning, workflow mapping, care-capacity modelling, caregiver redeployment discussion and pre-assessment of operational feasibility. It should not be used as a final staffing decision, cost-saving proof or commercial performance forecast.
6. How is the FTE estimate derived?
Q6. What methodology is used to derive the FTE-equivalent estimate?
The RR-Care™ framework uses a structured task-to-time-to-FTE conversion logic.
The process generally involves the following steps. The detailed calculation should be read together with the related technical paper, including task categories, operating-hour assumptions, demand constraints, supervision boundaries and recalibration requirements:
-
identifying routine task domains that may be robot-supported;
-
estimating the time associated with those routine tasks;
-
mapping robot-supported task activity against baseline caregiver workload;
-
applying defined operating-hour assumptions;
-
applying demand constraints;
-
considering human supervision and workflow boundaries;
-
converting released routine workload time into an FTE-equivalent planning indicator.
The simplified logic is:
robot-supported routine task time → released routine workload → FTE-equivalent planning indicator.
This is a framework calculation. It is not a clinical trial outcome, not a staffing order and not a final institutional deployment decision.
7. What types of tasks are included?
Q7. What task domains may be considered in RR-Care™?
RR-Care™ focuses on routine, repeatable, supervised and institutionally bounded care-support tasks.
Examples may include:
-
routine monitoring and reminders;
-
basic delivery or item-transfer support;
-
wayfinding or mobility-related assistance under supervision;
-
routine companionship or interaction support;
-
environmental or workflow-support observations;
-
scheduled check-in or alert-support activities;
-
task support that reduces repeated caregiver rounds.
-
These task domains must be interpreted cautiously. RR-Care™ does not claim that robots replace professional nursing care, clinical judgment, emotional care, emergency decision-making or human responsibility.
The framework focuses on routine workload support, not autonomous clinical care.
8. What does RR-Care™ not measure?
Q8. What should readers not infer from RR-Care™?
Readers should not infer that RR-Care™ proves:
-
improved clinical outcomes;
-
reduced mortality or morbidity;
-
improved medical treatment;
-
resident psychological improvement;
-
regulatory approval;
-
universal safety;
-
confirmed cost savings;
-
guaranteed headcount reduction;
-
product certification;
-
commercial success;
-
general applicability to all care settings.
The framework is designed to support structured planning and future validation. It does not replace clinical evaluation, professional judgment, institutional governance review or regulatory assessment.
9. What evidence supports RR-Care™?
Q9. Where do the data and evidence materials come from?
The RR-Care™ framework may be supported by a combination of:
-
anonymised and aggregated operational observations;
-
task-level workflow mapping;
-
robot-supported routine task categories;
-
caregiver workload assumptions;
-
system or operating-log references where available;
-
internal evidence-control materials retained for authorised review;
-
public academic and institutional literature used for contextual positioning.
The public version should not disclose personally identifiable resident data, identifiable medical records, biometric identification data, individual clinical decision data, confidential facility data, raw staff signatures or sensitive operational records.
The correct public interpretation is:
The supporting materials are anonymised, aggregated or internally retained under access-controlled conditions. Identifiable resident, caregiver, facility or commercially sensitive source records are not intended for public disclosure.
10. Is RR-Care™ a clinical study?
Q10. Does RR-Care™ constitute clinical validation?
No.
RR-Care™ is not a clinical trial, clinical validation report, medical diagnosis study, treatment evaluation or resident outcome study.
It does not claim to prove:
-
clinical effectiveness;
-
medical treatment value;
-
resident health improvement;
-
diagnostic accuracy;
-
therapeutic benefit;
-
clinical safety clearance.
-
RR-Care™ should be understood as:
a framework-level research and workload-planning model for robot-supported routine care-capacity release under defined assumptions.
If future empirical studies involve identifiable personal data, vulnerable elderly residents, health-related data, clinical evaluation or human participants, separate ethics review, consent procedures, data-protection safeguards and regulatory review would be required.
11. Is RR-Care™ a regulatory approval or product certification?
Q11. Does RR-Care™ approve the robot for deployment?
No.
RR-Care™ does not constitute or replace:
-
regulatory approval;
-
medical-device clearance;
-
product certification;
-
clinical evaluation;
-
institutional ethics review;
-
data-protection assessment;
-
legal review;
-
professional care judgment;
-
site-specific deployment approval.
The framework may support planning, internal review, institutional discussion and future validation, but it does not authorise deployment.
The safe interpretation is:
RR-Care™ provides a structured workload-release and care-capacity planning framework. It does not constitute regulatory approval, clinical validation, medical-device certification or institutional deployment approval.
12. Is RR-Care™ a literature review?
Q12. Is RR-Care™ based on a systematic literature review?
RR-Care™ should not be described as a full systematic review unless the work separately follows a formal systematic-review protocol such as PRISMA.
The safer description is:
RR-Care™ includes public-source literature and institutional-source review for contextual positioning, but its main contribution is framework development and demonstration calculation, not a standalone systematic review.
The literature component may include public academic and institutional sources related to eldercare robotics, assistive robotics, nursing-home technology, caregiver workload, workflow support, AI governance, human supervision and institutional deployment.
The FTE-equivalent estimate itself is not a pooled meta-analysis result. It is derived from the RR-Care™ framework calculation and demonstration assumptions.
13. What methodology does RR-Care™ use?
Q13. What are the main methodological layers?
RR-Care™ can be explained through two main methodological layers.
Methodology 1: Task-to-time-to-FTE conversion
This method maps robot-supported routine task domains into estimated caregiver workload-release time. It then converts the released routine workload into an FTE-equivalent planning indicator using defined working-hour and demand assumptions.
It focuses on:
-
task categories;
-
task frequency;
-
robot-supported time;
-
caregiver baseline workload;
-
operating-hour assumptions;
-
demand constraints;
-
human supervision boundaries.
Methodology 2: Evidence-control and governance-boundary assessment
This method checks whether the workload-release calculation is supported by reasonable evidence boundaries, including:
-
source-record traceability;
-
anonymised and aggregated evidence;
-
workflow plausibility;
-
supervision requirements;
-
safety and governance controls;
-
limitations and recalibration needs.
Together, these two methodological layers allow RR-Care™ to provide a structured workload-release estimate while preserving caution about evidence quality, local applicability and governance requirements.
14. How should engineers read RR-Care™?
Q14. What does RR-Care™ mean for engineering teams?
For engineers, RR-Care™ highlights that care robotics deployment is not only about whether a robot can technically perform a task. It is also about whether the task can be integrated into a real institutional workflow under human supervision.
Engineering teams may use RR-Care™ to consider:
-
task reliability;
-
operating-hour assumptions;
-
system uptime;
-
handover between robot and staff;
-
alert burden;
-
human override;
-
error handling;
-
navigation constraints;
-
maintenance burden;
-
logging and reviewability;
-
workflow integration.
The framework encourages engineering teams to design systems that support measurable, auditable and institutionally usable routine care-support functions.
15. How should medical and care professionals read RR-Care™?
Q15. What does RR-Care™ mean for medical and care professionals?
Medical and care professionals should interpret RR-Care™ as a workload-planning and care-capacity framework, not as a replacement for professional care judgment.
The framework may help care professionals consider:
-
which routine tasks may be safely supported by robots;
-
which tasks must remain human-led;
-
where supervision is required;
-
how caregiver time may be released;
-
whether released time can be redirected to higher-value care;
-
how resident-facing risks are managed;
-
how escalation and incident handling are documented.
RR-Care™ does not claim that robots replace human empathy, nursing judgment, clinical assessment, emergency response or professional responsibility.
16. How should government agencies and eldercare institutions read RR-Care™?
Q16. What is the relevance for public-sector and institutional readers?
Government agencies and eldercare institutions may read RR-Care™ as a structured research framework for thinking about how AI-enabled eldercare robots may affect routine workload and care-capacity planning.
The framework may support discussion on:
-
institutional workload planning;
-
responsible adoption of care-support robotics;
-
pilot design;
-
human supervision;
-
evidence collection;
-
care-capacity reallocation;
-
governance safeguards;
-
limitations of automation;
-
future validation needs.
It should not be used as a substitute for official policy decisions, regulatory assessment, procurement due diligence, clinical evaluation, data-protection review or institution-specific approval.
17. Why is RR-Care™ relevant to investors and shareholders?
Q17. Why does RR-Care™ matter if it is not commercial validation?
RR-Care™ is relevant because it provides a structured research foundation for assessing the potential institutional value of AI-enabled eldercare robotics.
Its relevance lies in:
-
creating a defensible research framework;
-
clarifying how routine workload release may be measured;
-
supporting future discussions with institutions, healthcare partners, regulators and researchers;
-
reducing the risk of unsupported commercial claims;
-
demonstrating that the company is developing structured evidence-based deployment logic;
-
supporting future peer-reviewed research, institutional pilots and responsible commercial evaluation.
However, RR-Care™ should not be presented as proof of revenue, guaranteed cost savings, clinical approval, confirmed staffing reduction or commercial success.
The safe shareholder-related interpretation is:
RR-Care™ provides a structured research and assessment foundation for future institutional engagement and responsible commercial evaluation. It is not itself a commercialisation result, sales forecast or staffing-reduction commitment.
18. Is RR-Care™ proprietary?
Q18. Is RR-Care™ a company-developed framework?
RR-Care™ may be described as a company-developed research and assessment framework.
However, it should not be presented as a closed commercial product unless separate intellectual property, licensing, regulatory, commercialisation or productisation steps are formally established.
The safe interpretation is:
RR-Care™ is a company-developed research and assessment framework that may be further refined, validated, published and applied in future research, institutional engagement and responsible deployment assessment.
19. Can RR-Care™ be submitted to a peer-reviewed journal later?
Q19. Can the framework later be developed into a journal manuscript?
Potentially yes, subject to the target journal’s policies.
Any future journal submission should:
-
disclose any prior public company website version or DOI;
-
explain that the prior version was a non-peer-reviewed technical preprint or technical disclosure;
-
substantially revise and strengthen the manuscript;
-
add further scholarly value;
-
include stronger methodology, literature positioning, validation, sensitivity analysis or independent review where applicable;
-
comply with the journal’s prior-publication and preprint policy.
The company website version should not describe itself as a journal article, accepted manuscript, final publication, regulatory approval or product-clearance document.
20. What are the main limitations of RR-Care™?
Q20. What should readers keep in mind?
The key limitations are:
-
the current version is not independently peer-reviewed unless later accepted by a journal;
-
the FTE estimate is based on defined assumptions and evidence boundaries;
-
FTE = 2.3 is illustrative, not universal;
-
local workflow recalibration is required;
-
evidence quality depends on source-record completeness and reviewability;
-
multi-site validation remains necessary;
-
longer deployment periods are needed;
-
independent assessor review would strengthen credibility;
-
clinical effectiveness and resident outcome improvement are not established;
-
commercial viability and revenue generation are not established.
-
detailed task-frequency, operating-hour and supervision-time assumptions should be reviewed before institutional application;
-
pilot-site verification is required before any operational, procurement or staffing-related interpretation.
These limitations should be treated as part of responsible public disclosure, not as issues to hide.
21. What should not be concluded from RR-Care™?
Q21. What interpretations should readers avoid?
Readers should avoid concluding that:
-
one robot replaces 2.3 caregivers;
-
FTE = 2.3 is a universal staffing benchmark;
-
the framework proves cost savings;
-
the robot is clinically validated;
-
the robot is approved for deployment;
-
the company has achieved regulatory clearance;
-
the framework guarantees commercialisation;
-
the study proves staffing reduction;
-
the result applies to all nursing homes;
-
the result is a final peer-reviewed conclusion, unless later accepted and published by a peer-reviewed journal.
Preferred interpretation:
RR-Care™ is a framework-derived, context-specific workload-release and care-capacity planning model under defined assumptions and evidence boundaries.
22. What is the safest one-sentence summary?
Q22. How should RR-Care™ be summarised?
The safest one-sentence summary is:
RR-Care™ is a company-developed, non-peer-reviewed research and planning framework that estimates robot-supported routine workload-release capacity in institutional eldercare settings under defined assumptions, but it does not constitute clinical validation, regulatory approval, staffing-reduction authorisation, commercial valuation or universal deployment readiness.
23. Public-facing conclusion
RR-Care™ is proposed as a structured research and planning framework for evaluating robot-supported routine workload release in institutional eldercare settings. It is intended to support responsible discussion among care institutions, engineers, healthcare professionals, governance reviewers, researchers and interested public stakeholders.
Its contribution is to translate selected robot-supported routine task activity into a framework-level FTE-equivalent care-capacity planning indicator under defined assumptions and supervision boundaries.
The illustrative FTE = 2.3 estimate should be interpreted only within its stated assumptions and evidence boundary. It indicates a possible workload-release planning estimate for further assessment, not staff replacement, regulatory approval, clinical validation, guaranteed cost savings or universal deployment readiness.
Final Public Interpretation Statement
RR-Care™ should be understood as:
a framework-level routine workload-release and care-capacity planning model, not regulatory approval, clinical validation, staff-replacement authorisation or commercial valuation.